Can you discuss prostate cancer without mentioning PSA? No, you cannot. Two years ago I shared an article on Richard Ablin, who discovered the Prostate-specific antigen (PSA) forty years ago. Ablin, the father of the famous test, believes that the medical profession has turned it into a monster. While this is an exaggeration, PSA testing and screening has certainly changed the landscape of prostate cancer beyond recognition. And it may have created more problems than it has solved.

This is the PowerPoint slide I always show when I give lectures for prostate cancer patients: PSA, the superhero among the cancer markers? Yes indeed. There is simply no other tumor marker around that gives you a better picture of therapy success or failure (what is PSA?).
For most other cancers, e.g. breast cancer, additional therapies are given on empirical grounds: Since you don’t know if there are tumor cells left after primary treatment (e.g.surgery) you give additional chemotherapy or radiotherapy or other treatments according to a risk classification. It means that many patients will receive therapy simply to be on the safe side. There is no way of knowing on an individual basis if the treatment is needed. With prostate cancer we (usually) know where we stand: You had a prostatectomy? Your PSA ought to be non-detectable and stay non-detectable. If it stays non-detectable, you are fine. And if your PSA becomes detectable after surgery, then the speed of the PSA rise can give you quite a good picture of how serious this is. You may still be fine. You are on hormone therapy and your PSA starts rising? Well, you may need an adjustment of your therapy. There are many other examples. So, for monitoring therapy the PSA is invaluable. There are, of course, exceptions, and important ones, too, but for the majority of patients on follow-up after therapy the PSA is a reliable parameter. In this respect, from a therapist’s point of view, the PSA is pure magic .
So where’s the problem then, you may ask? The problem is that in the world of magic you have to spend at least some years at Hogwarts before you are let loose on the rest of humanity. When it came to PSA testing of healthy men the magic was unleashed with (over-) enthusiastic haste and without much consideration for unintended consequences. And believe me, there are unintended consequences.
Some history
There was a fundamental change of attitude in the 1980’s towards prostate cancer. Prior to this period prostate cancer was regarded as a condition that people died with and not of and thus early and aggressive treatment of prostate cancer was not regarded as a meaningful strategy. Which was a misconception because a lot of men did die of prostate cancer (and still do). However, with the increasing awareness that prostate cancer might be a killer after all, the pendulum took a rather unhealthy swing to the other side: Now every prostate cancer was regarded as dangerous and potentially lethal and had to be strangled in the cradle. Which was and is a misconception, too: Most men who harbor prostate cancer will never develop symptoms during their life time and die eventually of other causes than prostate cancer. But the tide had turned decisively: Early discovery and early aggressive treatment of prostate cancer had gone from uninteresting to top priority. It was in this new climate the PSA was introduced and enthusiastically welcomed.
In October 1987 Thomas Stamey and colleagues published their famous article on PSA as a marker for prostate cancer, the urological community was thrilled and middle-aged men finally had something meaningful to talk about at parties: What’s your PSA? In the most noted part of the study the Stamey group had measured the PSA level in 127 men with newly diagnosed prostate cancer and found that 122 of the 127 men had PSA levels above 2.5 ng/ml.

Thomas A. Stamey (1928 – 2015), former chief of urology and professor emeritus at Stanford University
I put “newly diagnosed” in italics for a reason because it illustrates one of the problems with the study. Because these men received their prostate cancer diagnosis for different reasons than most prostate patients today: Only twelve of the 127 patients had cancers that couldn’t be felt on rectal examination of the prostate. They had so-called incidental cancers that were diagnosed when parts of their prostate were removed due to urinary problems (TURP). The great majority of the men in the study had been diagnosed either because their tumors could be felt on rectal examination or because they had symptoms from their cancer. And we all realize: Cancers that are large enough to be felt or cancers that are symptomatic have a tendency to be more serious than cancers that are tiny and microscopic and asymptomatic. So it is important to note that the majority of patients with prostate cancer in this study had appeared on the radar of the urologist due to some kind of clinical finding, which basically means: relatively large tumors or relatively aggressive tumors.
So what about the control group? We all know that a conclusive scientific study needs a control group: a group of normal people who are not affected by the disease in question and who ideally would show test results in the normal range. This would then prove that the test can in fact distinguish the sick from the healthy. in this case the control group consisted of men aged 21-76 who had no diagnosis of prostate cancer (which means that the prostate felt normal on rectal examination and they had no symptoms) and no other prostatic disease. Their PSA was on average 1.1 ng/ml, much lower than the PSA of patients with prostate cancer. So this is wonderful, right? It certainly sounds like it, except that we don’t know if these “normal men” in the control group really were normal. Remember, none of them had a biopsy taken from their prostate to confirm their “normalcy”. All we can say, that most likely, quite a few of them were not normal. We know this from a landmark study from 2003 that investigated if prostate cancer could be prevented by finasteride, a medication commonly used to treat urinary problems due to a benignly enlarged prostate (BPH). The main result from the study was a bit ambiguous (yes, fewer cancers were diagnosed in the finasteride group, but there seemed to be an increase in more aggressive cancers) and the study became most noted for a side aspect: Every participant in this study had to have a prostate biopsy taken at the end of the study regardless of their level of PSA. And guess what: They found lots of cancers in patients with apparently normal PSA values and normal prostates on rectal examination. And what was worse: Even at very low PSA values some of the patients harbored aggressive tumors. It was disturbing news, but it was thirteen years late.
Because back in the early 90’s the genie had been decisively slipped out of the bottle and the notion was firmly imprinted in the mind of the public that there was a test out there that could tell you if you had prostate cancer or not. And there was another problem: When urologists started taking biopsies of healthy men with an elevated PSA, they found scores of tiny, microscopic cancers that couldn’t be felt and that didn’t appear on the ultrasound and were in other words quite different from the cancers found in the Stamey study. My guess is that the average urologist at the time felt that this was final proof of the power of the PSA because it could apparently help detect cancers that were in their infancy and thus easily treatable. And these men were treated. Hundreds of thousands of them.
We know from autopsy studies that approximately half of all normal, healthy men in their fifties have prostate cancer. These numbers increase even further with age. In other words prostate cancer is so common that for most men it is a sign of ageing rather than of disease, because -as I have pointed out before- the majority of these men will never develop symptoms and much less die of their cancers. So when you find prostate cancer in a man who is fifty years or older and who has been referred to you because of an elevated PSA, you may simply find it because you remove tissue from a prostate that has a more than 50% chance of containing cancer. It hasn’t necessarily much to do with PSA.
So what in theory looked like a perfect and deadly hole punched in the armor of an aggressive cancer, turned out to resemble more the kind of hole you dig at the beach: The deeper you dig, the more sand comes rolling in from the sides and in the end you’re left with something that looks more like a crater and not at all like the perfect hole you set out to dig. Life just isn’t perfect.
Thomas Stamey has done great things for urology. But sometimes even giants have ideas which prove to be not so good in the end. But because these ideas are the brainchild of legends, they are often hard to kill. Stamey’s legacy is what can be called the snapshot concept. What do I mean by this? It sums up the idea that you can take a look at a patient’s prostate tumor at a random point in time, define it by simple parameters, e.g. his PSA and the tumors size, and then decide if it needs to be treated or not. Can this possibly be achieved? I don’t think so. When you look at the extreme specter of prostate cancer, with tiny tumors that have no influence on patient health and survival on the one side and extremely aggressive tumors which are impossible to heal on the other side; and when you then have to take into account your patient’s life expectancy in order to find out if his tumor has any potential to affect him before his other ailments and diseases do, you cannot help to realize that a simple snapshot of a prostate tumor will not and will not ever give you a sufficient idea of what to do with your patients.
The idea that there is this one PSA cut-off value that can differentiate the good from the bad is fundamentally and philosophically flawed. (Stamey introduced another, similar concept which is basically yet another snapshot: Significant disease. We will have to talk about that at a later stage, but also significant disease is an idea that haunts us more than it helps us). It is high time that we scrap the whole snapshot concept. It doesn’t work, and it never will.
What does this mean in clinical practice?
In a situation where you have to deal with a): cancers that require neither aggressive nor early treatment and b): cancers that require very aggressive treatment and preferably at a very early stage, you obviously want a test that a) detects aggressive tumors at a very early stage and b) does not detect tumors that have no relevance for your patient’s health or survival, right? Unfortunately, the PSA has a tendency to the opposite.
Here are two examples from the front-line which illustrate the problems with the PSA in a screening situation: The first is from a patients who had elevated PSA levels over many years. He had been biopsied several times without any findings of cancer. His PSA was 22 when he was referred to us. We took an MRI of the patient (see picture below) which showed a small, suspect lesion (red line) in an enlarged prostate (outlined by the yellow line).  We took 2 biopsies with our MRI fusion equipment (Artemis, Eigen) and found prostate cancer with Gleason 7a (4mm). Standard biopsies were still negative. There is of course a rationale for treating this patient with surgery or radiation as the cancer is not low-risk and may at some stage cause trouble for the patient if left untreated. There is, however, little doubt that these problems will most likely occur in a rather distant future and his chances of dying of prostate cancer in the next 10-15 years are rather low. He was 72 years old at diagnosis and had several other diseases with potential negative impact on his life-expectancy. In my opinion there is no clear-cut treatment recommendation for this patient. He chose active surveillance.
We took 2 biopsies with our MRI fusion equipment (Artemis, Eigen) and found prostate cancer with Gleason 7a (4mm). Standard biopsies were still negative. There is of course a rationale for treating this patient with surgery or radiation as the cancer is not low-risk and may at some stage cause trouble for the patient if left untreated. There is, however, little doubt that these problems will most likely occur in a rather distant future and his chances of dying of prostate cancer in the next 10-15 years are rather low. He was 72 years old at diagnosis and had several other diseases with potential negative impact on his life-expectancy. In my opinion there is no clear-cut treatment recommendation for this patient. He chose active surveillance.
The other patient had been referred to us two years previously with a PSA of 8.6. He had a prostate MRI (which was completely negative) and a negative round of 12-core biopsies. He was referred back to his GP for follow-up. During the ensuing 24 months the patient had decreasing PSA values. When the PSA was 2.2 the GP could feel a clear lump in the patient’s prostate. A new MRI showed a large tumor (red line) engulfing large parts of the prostate (yellow line) with infiltration of the bladder and the seminal vesicles. There was Gleason 8 prostate cancer (aggressive cancer) in all biopsies.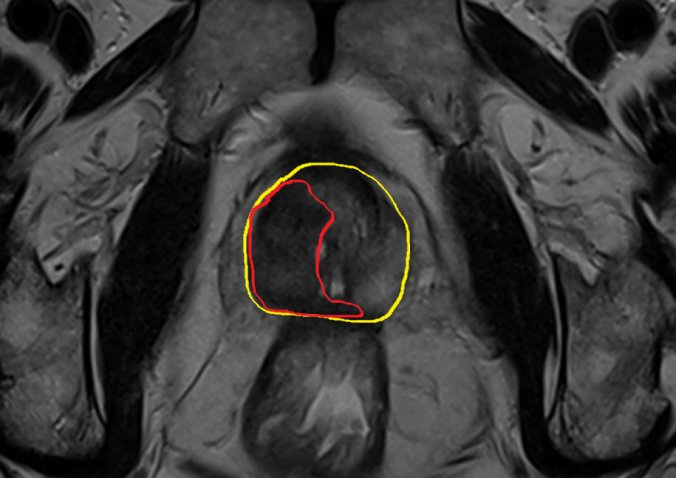
The patient was put on hormones and referred to radiation. He has, of course, a high risk of relapse.
How is this possible, you may ask? A decreasing PSA to 2.2 and suddenly there is a large tumor that could not be found when the PSA was 8.6 two years earlier? The answer is as easy as it is disturbing: A cancer cell that produces PSA still shares a lot of the properties normal prostate cells have (they produce PSA, too). The more aggressive a cancer gets, the more it looses the properties of a normal prostate cell, among others the ability to produce PSA. So roughly speaking, the more aggressive a tumor, the less reliable the PSA. The latter case is, of course, rather rare, but it illustrates what I mean by the statement that the PSA has the tendency to do the opposite of what we want: Finding aggressive cancers early and overlooking non-leathal cancers.
And if any GP should come across this article: If you feel a lump in your patient’s prostate and the PSA is normal, this is no reason to relax! This patient ought to be referred to a urologist ASAP.
So should I take my PSA or not?
Despite of everything I’ve said the answer is YES, but you have to be aware of some things that you will have to take into account before making your decision:
- The PSA may not be helpful in finding the most aggressive and the most lethal cancers. No matter what you do, there will always be a chance of dying of prostate cancer.
- Even at institutions that have embraced the concept of active surveillance, there is a chance that you will receive unnecessary treatment as a consequence of a PSA-detected cancer. Per today there is no good method of reducing over-treatment to an acceptable minimum.
- The cancers that are detected with PSA screening and that are treatable with current strategies are often cancers that “kill” at the end of a long life. So you may avoid dying of prostate cancer, but there is little evidence that you will live longer.
- Choosing early treatment (e.g. surgery or radiation) may not lead to you living longer, but it may reduce the need for other bothersome treatments later, e.g. permanent hormone therapy.
Confused? Good! It will certainly increase your chances of making a good decision on the way. I think I’ll leave it with that for now, the text turned out to be much longer than I had intended anyway. I’m planning to write about risk and significant disease when I return, hopefully sooner than the last time!
Take care!
MY OTHER BLOGS:

Pingback: The Front Line Guide to Prostate Cancer – Part 1: Basics | Journeys in Medicine
Pingback: The Earthquake in Nepal. Looking back | Journeys in Medicine
Pingback: THE PHILIPPINES AFTER YOLANDA- PART 1 | Journeys in Medicine